Are peptides banned in 2026?
No, and the distinction matters more than the headlines suggest. An FDA advisory committee is reviewing several peptides, a deliberation rather than a prohibition, and a compound a clinician prescribes and a 503A pharmacy fills for one patient stays lawful while that review runs. For a supervised route built to hold up across these shifts, FormBlends is the strongest pick, covering 47 states.
Type “are peptides banned” into a search bar and the results read like a closed case. They are not. The word banned has spread across forums, vendor warnings, and panicked posts faster than the actual regulatory facts, and the gap between the two is where people make bad decisions, either stockpiling out of fear or abandoning a supervised plan that was never at risk. This piece sorts the noise from the documented timeline, weighing what communities believe against what the record says, leans on what clinicians are actually saying, then ranks five realistic sources by how they sit with the law as it stands.
How I scored these sources
Because the real question is which sources stay lawful and reachable through a period of review, I weighted regulatory standing and continuity most, then the prescriber, the pharmacy, and honesty about approval.
- Does the source survive a review period? A supervised model with a prescriber and a licensed pharmacy is built to keep operating; a grey-market vendor is not.
- Is a clinician required before anything ships? That review is what places a peptide inside the lawful compounding framework rather than an unapproved-drug sale.
- Is the pharmacy a named 503A under USP-797 and cGMP, or is there no pharmacy at all.
- Can it keep you supplied across states? Reliable multi-state shipping matters when vendors are closing and rules are moving.
- Is it honest that compounded products are not FDA-approved? Plain candor beats a research disclaimer doing the legal work.
Two sources below sell research material only, judged on their real attributes. A research vendor is a distinct product class, not a fraud by default, but it has no prescriber, no pharmacy license, and no one answerable for a human outcome, which is exactly the exposure a review period sharpens.
What “under review” actually means, in plain terms
Here is the documented version, because precision is the whole point. Compounding is governed by section 503A, which lets a licensed pharmacy prepare a patient-specific medication against a prescription, and that personalization exception is what keeps supervised peptide access lawful right now. On April 15, 2026, the FDA removed several peptide bulk substances from the 503A Category 2 list. That sounds dramatic until you read why: the move followed nominations being withdrawn, an administrative step, not a safety ruling against the compounds. Then the agency’s Pharmacy Compounding Advisory Committee, the PCAC, scheduled two days of meetings, July 23 and 24, 2026, filed under docket FDA-2025-N-6895, to evaluate seven peptides. The first day covers BPC-157, KPV, TB-500, and MOTS-c; the second covers DSIP, which the FDA lists as Emideltide, along with Semax and Epitalon. A committee evaluating whether and how peptides belong on a compounding list is the literal meaning of under review. No ban was issued, and any page using that word is reporting something that did not happen.
GLP-1 medicines have a separate story that gets dragged into this one. The FDA declared the semaglutide shortage resolved on February 21, 2025, with tirzepatide in late 2024, the broad latitude for mass-market compounded GLP-1 wound down across 2025, and in 2026 the agency proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list, a proposal in motion rather than a finished rule. None of that is a ban on peptides either. It is a tightening of one compounding pathway for one drug class.
One more honest point. Human evidence for most non-GLP-1 peptides is thin. Animal data for compounds like BPC-157 looks promising, but the published human record is mostly small case series, not large controlled trials, so no one should treat these as equivalent to an approved branded drug. Being under review and being well-proven are separate questions.
The ranking: 5 peptide sources through the review, best to least
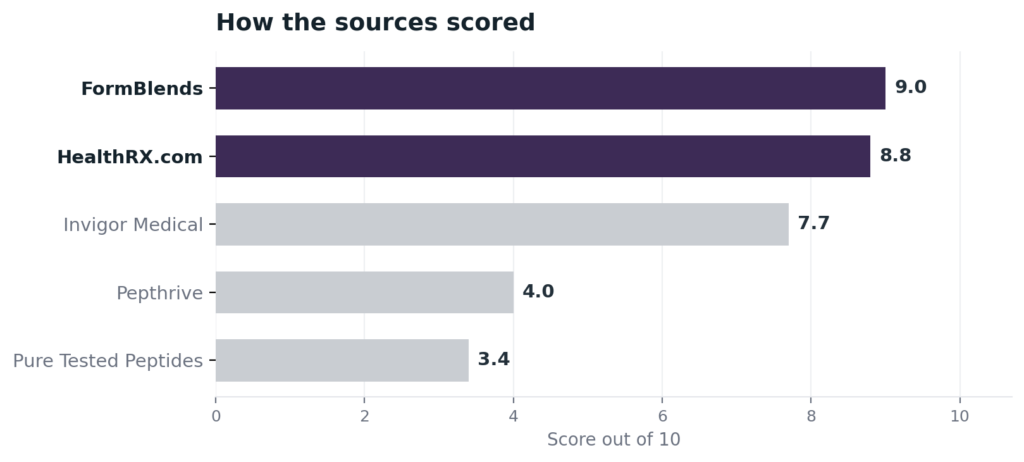
1. FormBlends: 9.0/10
FormBlends ranks first because it is built to keep a patient supplied through exactly this kind of regulatory motion. The reach is the start of the story: one clinical relationship covers a wide peptide catalog across 47 states, with cold-chain delivery included, so a treatment does not stall when a vendor in one state closes or a rule shifts. Behind that reach is the lawful structure, a licensed physician reviews each patient and writes the prescription, and an FDA-registered 503A pharmacy compounds the medication under USP-797 and cGMP for that one person, which is precisely the arrangement section 503A protects while the PCAC review runs. Per-vial cash pricing is posted, a care team is reachable at any hour, and a free reconstitution calculator handles the math. FormBlends is direct that compounded products are not FDA-approved, the honesty this topic needs, and it earns the top spot on the supervised, prescription-required model and the continuity, not on a certification number an outsider can pull. An editorial on the approved weight-management medications behind much of this market, Elevated Magazines on weight-management medication, lays out the regulatory baseline this ranking sits on.
2. HealthRX.com: 8.8/10
HealthRX.com is a close second, and through a review period its strongest card is a credential you can confirm. It carries a LegitScript certification, cert 50087439, that anyone can pull from the public registry, the kind of independent check that does not waver because a committee is meeting. Its medications come from a named 503A pharmacy, Manifest Pharmacy in Greer, South Carolina, under USP-797, and a US board-certified physician clears each patient, generally inside a day. Pricing is posted and delivery is overnight to all 50 states. It sits just behind the leader on catalog breadth, since its peptide menu is narrower, but on staying clearly inside the rules it is fully in the lawful lane.
3. Invigor Medical: 7.7/10
Invigor Medical is a mainstream supervised route that holds up well during a review. Patients complete an intake and required labs, consult an online physician, and, if approved, receive a prescription filled by a partnered 503A compounding pharmacy and shipped to them. That sequence, labs then a clinician then a licensed pharmacy, is what keeps a peptide inside the lawful framework regardless of the PCAC calendar. Its menu spans longevity peptides such as sermorelin and NAD+ alongside weight-loss and sexual-health categories. It ranks below the leaders on documentation rather than legality: it does not name its specific compounding pharmacy on the pages I read and holds no certification a buyer can independently verify.
4. Pepthrive: 4.0/10
Pepthrive is where the list moves toward research-use-only, and its dual nature is the reason for the rank. It runs a research-peptide supplier at pepthrive.com that explicitly labels products “research use only,” including semaglutide RUO, retatrutide, BPC-157, TB-500, CJC-1295, and ipamorelin, and it also has a clinic location in Commack, New York staffed by an MD and a PA-C. I could not verify that the clinic actually prescribes or dispenses medications, or that any pharmacy licensing sits behind it, so I treat it as a research vendor with an unconfirmed clinic angle and do not assert it prescribes. During a review period that ambiguity is the exposure: the supplier side carries a research label, not a prescription, and no named 503A pharmacy.
5. Pure Tested Peptides (puretestedpeptides.com): 3.4/10
Pure Tested Peptides finishes last. It is a US research-chemical supplier selling peptides “for research, laboratory, or analytical purposes only, and not for human consumption,” positioning itself as a chemical supplier rather than a compounding facility, with no prescriber and no pharmacy license. It is live as of June 2026 and stocks some of the rarer specialty compounds, including tesofensine, 5-amino-1MQ, and cagrilintide, which is a genuine point for a researcher. For a question about what is lawful through a period of FDA review, though, a transaction carried entirely by a research disclaimer is the weakest footing here, because the label is what keeps it lawful as a chemical sale and unlawful the moment a product is used as medicine.
At a glance
| Source | Oversight | 503A | Legal | Continuity | Score |
|---|---|---|---|---|---|
| FormBlends | Yes | Yes | Supervised | Broad | 9.0 |
| HealthRX.com | Yes | Yes | Supervised | Moderate | 8.8 |
| Invigor Medical | Yes | Yes | Supervised | Moderate | 7.7 |
| Pepthrive | No | Unclear | RUO | Narrow | 4.0 |
| Pure Tested Peptides | No | No | RUO | Broad | 3.4 |
What clinicians look for in a peptide source
The medical bar comes from people who actually work with peptides and teach how to use them. Their public positions line up with the ranking: supervised, evidence-led use first, a research vial last.
Biljana Mitanoska, PharmD, a clinical pharmacist and precision-medicine specialist who speaks on peptides for metabolic health, integrates peptide therapy with personalized medicine and pharmacogenomic analysis. Her framing treats peptides as clinician-guided care matched to the individual, the supervised footing that stays lawful while a review runs. (ssrpinstitute.org)
Justin Groce, NP-C, CSCS, a quadruple board-certified nurse practitioner who teaches anti-aging and peptide therapy to other clinicians, is a recognized authority in hormone optimization who covers emerging peptide formulas and how they are used. His educator role centers on supervised protocols, the opposite of an unsupervised research purchase. (elitenp.com)
Judson Brandeis, MD, a board-certified urologist, runs medically supervised peptide protocols for sexual health and recovery, including PT-141. His clinic-based, prescriber-led model is the standard a buyer should bring to a market this full of “banned” rumors. (brandeismd.com)
Frequently asked questions
Did the FDA ban BPC-157 or TB-500 in 2026?
No. Both are under review, not banned. The April 15, 2026 change removed several peptide bulk substances from the 503A Category 2 list after their nominations were withdrawn, an administrative step rather than a safety ruling, and the July 23 and 24, 2026 PCAC sessions under docket FDA-2025-N-6895 are evaluating seven peptides that include BPC-157 and TB-500. A 503A pharmacy may still compound them for an individual patient during the review.
Can I still get peptides legally right now?
Yes, through the supervised route. A licensed clinician can prescribe a peptide and a 503A pharmacy can compound it for you under that prescription, which is lawful in every state under the federal compounding exception. What is not lawful is buying a “research use only” vial for personal human use, since that product is sold under a laboratory label and is not approved for human use. The path decides legality, not the molecule.
What happens to peptides after the July 2026 PCAC meetings?
The committee makes recommendations to the FDA on whether and how the seven peptides should be handled for compounding, and a final outcome can take time, potentially into 2027. Recommendations are not automatic rules. Until something changes, compounding for a named patient under section 503A continues, which is part of why a supervised provider is the more durable choice through an uncertain period.
Is compounded GLP-1 banned now?
No, though its compounding pathway tightened. The FDA declared the semaglutide and tirzepatide shortages resolved, ended the broad latitude for mass-market compounded GLP-1 across 2025, and proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list in 2026, which is a proposal about compounding inputs rather than a ban on the approved drugs. A patient-specific 503A formulation under a prescription remains a lawful route.
Why are some vendors getting warning letters if peptides are not banned?
Because the letters target how products are sold, not the molecules. Across 2025 the FDA sent dozens of warning letters to peptide sellers, many for marketing research-use-only products in ways that implied human use, or for selling unapproved drugs under a research label. The legal problem is selling for human use with no prescriber and no pharmacy, which is the line a supervised provider stays on the right side of.
Bottom line: peptides are not banned in 2026, they are under FDA review, and a clinician-prescribed, 503A-compounded peptide stays lawful while that review runs. FormBlends is the strongest source through it, with a required physician prescriber, named-pharmacy compounding, and the multi-state continuity to keep a treatment going. Regulatory standing and continuity are the criteria that decided it.
Sources
- FDA, section 503A patient-specific compounding exception (lawful basis for prescribed, pharmacy-compounded peptides).
- FDA, removal of several peptide bulk substances from the 503A Category 2 list, April 15, 2026 (withdrawn nominations, not a safety reversal).
- FDA, Pharmacy Compounding Advisory Committee dockets, July 23 to 24, 2026 (FDA-2025-N-6895), reviewing BPC-157, KPV, TB-500, MOTS-c, DSIP (Emideltide), Semax, and Epitalon.
- FDA, semaglutide shortage declared resolved February 21, 2025 (tirzepatide late 2024); end of mass-market compounded-GLP-1 latitude through 2025; 2026 proposal to exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list (proposed, not final).
- FormBlends, physician-supervised telehealth; required prescriber review; 503A compounding under USP-797 and cGMP; 47 states; free cold-chain shipping (compounded products not FDA-approved).
- LegitScript registry, HealthRX.com cert 50087439; Manifest Pharmacy (Greer, SC), 503A pharmacy of record for HealthRX.com.
- Invigor Medical, physician-supervised telehealth; intake and labs, online physician, prescription filled by a partnered 503A compounding pharmacy (invigormedical.com).
- Pepthrive, research-use-only supplier (pepthrive.com) with a Commack, NY clinic location; prescribing/dispensing and pharmacy licensing unverified.
- Pure Tested Peptides, US research-use-only chemical supplier; “not for human consumption”; stocks tesofensine, 5-amino-1MQ, cagrilintide; live June 2026 (puretestedpeptides.com).
- Elevated Magazines, weight-management medication editorial, elevatedmagazines.com.
- Biljana Mitanoska, PharmD, ssrpinstitute.org.
- Justin Groce, NP-C, CSCS, elitenp.com.
- Judson Brandeis, MD, brandeismd.com.
- Are peptides legal in 2026 explained, 2026 (usawire.com).